
Updated as of 09-18-2014 WHO report.
Many reports from on-the-ground workers with the WHO, Doctors Without Borders, state health and aid agencies, etc. have commented that the case and death rates in at least some locations have almost certainly been too low, because of a substantial number of people avoiding going to clinics and hospitals, out of fear primarily. This situation seems to be the worst in Liberia. See this article for example. Today’s WHO-released data from Liberia may be confirmation of this, many new cases and deaths being reported there from August 16-18. Such an explanation could be due to more intensive case tracking/finding. However, it is also possible that the epidemic is simply exploding there now, especially given that it is well established in the capitol of Monrovia. Or it could be due to some combination of the two.
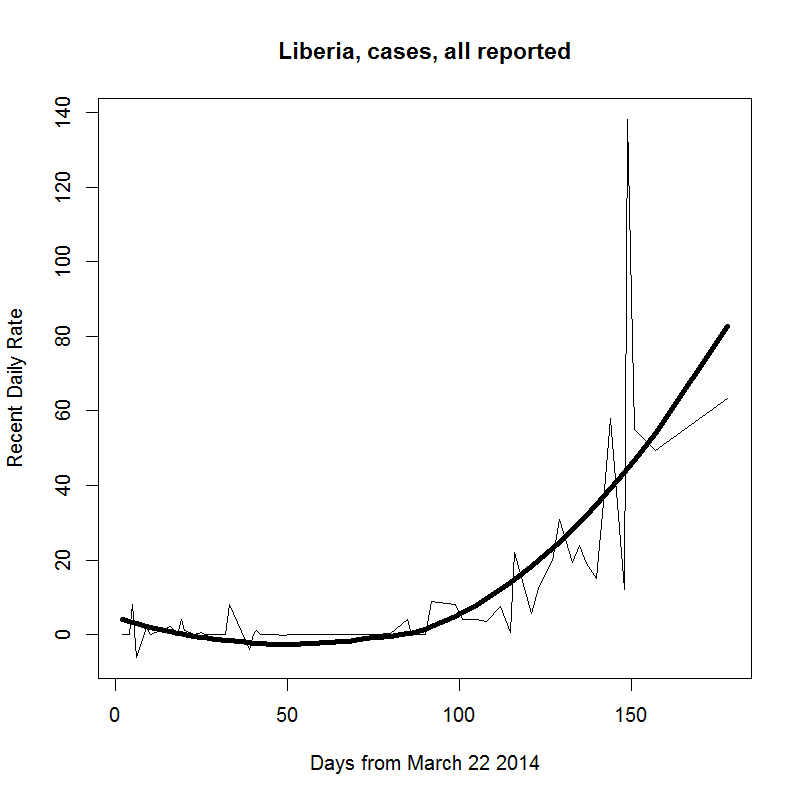
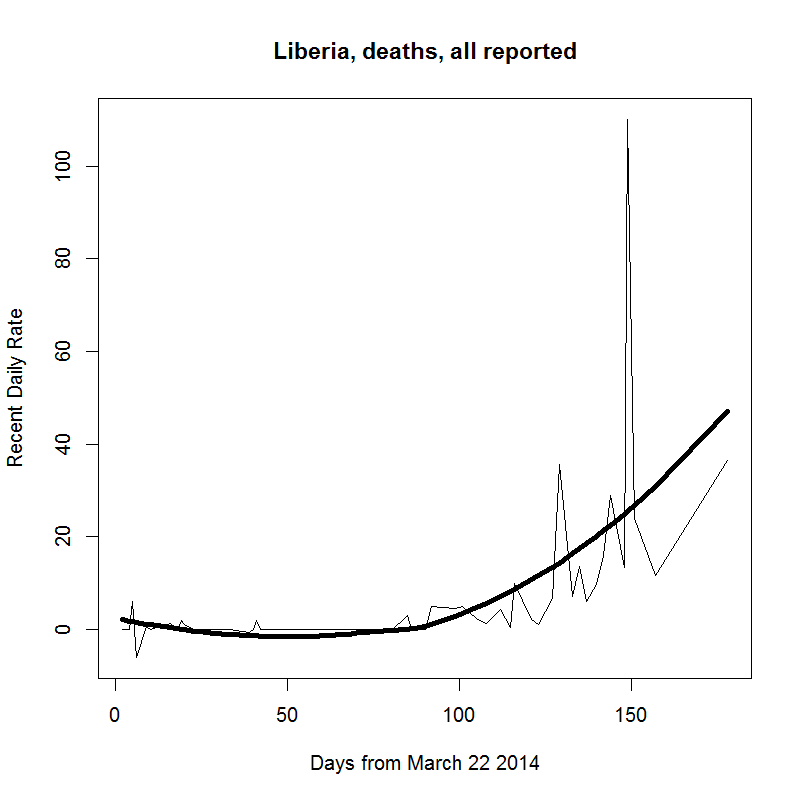
In the graphs below I used a pretty stiff “span” parameter (span = 1.0) in the loess smoothings (dark black lines) of the WHO-reported raw data (thin line). This choice gives about 35 deaths/day in Liberia. If I use something more flexible, span = 0.5 for example, the estimated rates are higher, about 47/day. However, it’s best to go stiff (i.e. conservative) here, because clearly there are major variations due to data gathering and reporting timelines that have been causing large fluctuations in the numbers (discussed more here). But there’s also clearly more than just that going on with this latest surge in numbers.
This situation is now extremely serious, if it wasn’t already. Note also that negative rates early on in the outbreak are presumably due to case retractions or re-classifications. Code generating data and graphs is here and data table itself is here.

By my understanding, the rise in infection & death rates is simply the result of uncontrolled infection in a more densely populated environment. Monrovia is the 1st large city (pop ~ 1 million) to have an uncontrolled ebola epidemic in the region.
This could soon be surpassed by the Lagos (pop ~ 25 million) infection node if contact tracing & quarantine fails there; the number of cases is now rising there.
A slow motion train-wreck.
I’ve not been able to find spatially specific data (beyond country by country), but yeah, no question that Monrovia has to be a gigantic concern. On the other hand, perhaps there will be less of the outright distrust of medical facilities that is causing the rural people to avoid them, thereby spreading the disease to family members and others (and also going unreported). That’s the hope anyway.
As for Nigeria, there were the original 12 contacts of the visitor who brought it in, but 3 new suspected cases were reported in the August 19 and 20 reports. So we’ll see what that means. Also hopeful is the fact that it never took off in Conakry, which is also a large urban area, albeit a different country.
Apparently the family of one of the dead nurses from the Patrick Sawyer case in Lagos was placed in unsupervised-home-quarantine but then bolted to parts unknown.
Clearly the situation in Monrovia is very bad when one of the only clinics present in town is attacked and looted of all including the sheets on beds. The army is currently enforcing the army version of quarantine in places but that may disintegrate if soldiers start getting infected. There have already been riots as a result. Trust will be hard to obtain in any of these countries, let alone ours. All you need to do is look at yahoo comments to see the many entries from nurses who will fail to show up once an infection goes positive where they work.
This is now getting expensive as hundreds of potential cases need to be quarantined for days and tested. I wonder why TPTB continue to allow commercial air travel & fail to quarantine these places (and let the hospitals bear the resulting costs).
I really should go re-read Camus “The Plague” for pointers – it’s been 40 years, heh.
Good points. I had forgotten about that incident regarding the hospital raid. Not a good sign for sure. And not only the cost for quarantine, but just the basic limitation on the number of hospital beds.
The raw data and the loess smoothings look somewhat parabolic. Hopefully, their shapes will change. Are there any models out there that could replicate the spread of this particular strain of Ebola? It would be interesting to see their output.
It is hard to fathom what it would be like to be quarantined in a slum like West Point with a virus that deadly. To a certain degree, it might make sense for the inhabitants to go ahead and try to escape because odds are ~60% that they are going to die if they contract Ebola. Yeah, that assumes a 100% infection rate. I don’t see many reasons not to assume a high rate of infection, though.
Assume that someone in West Point gets sick. The assumption is going to be made that they have Ebola even if they don’t. Will the authorities then transfer this individual to a clinic full of Ebola patients (assuming that there are any operational clinics left)? If all the person had was the flu, then they may have just gotten a death sentence. It seems to me that the inhabitants probably have plenty of good reasons not to report that they have gotten sick, which of course just makes the problem worse. What an absolute nightmare.
See the latest post for my estimates of spread rate and how I got them.
I don’t believe the strain (a variant of Zaire ebolavirus) matters hugely here, even if there are indeed differences in virulence between the four African strains. As for existing epidemiological modeling, I don’t know (I haven’t seen any), but the critical drivers are pretty clearly the behavior of the symptomatic (esp. how many people touch them), and the quality of the health care they receive. Certainly the former is very hard to predict in the current situation, and the latter cannot be very good. In the developed world those people would be in ICU units. There, they’re dying on cement and dirt floors because they’re more comfortable than the beds.
There will now have to be an international aid response it seems.
I suppose the really important question here now is why have previous outbreaks burned out relatively quickly? The recent history of civil war in all three countries probably contributed to the lack of an effective early response, but none of the previous epidemics have been in especially stable areas. My guess is that the close proximity of the three countries and ease of crossing borders has contributed to the spread and the lack of efficacy of control efforts. Now that it is in large urban areas it would seem to be very difficult to control.
It really does seem to be getting out of hand and one does have to wonder what the virus genomes may be up to in such a large population of infected people. There is also an outbreak of ‘haemorrhagic gastritis’ (allegedly not Ebola and with only a 12% mortality rate being reported) in Zaire near the original source of this Ebola strain. Seems to be one of those interesting times mentioned in the possibly apocryphal Chinese curse.
In Zaire, apparently Mobutu’s strict quarantine of Kikwit kept it out of Kinshasha, at least in the second major outbreak in the 1990s. I’ve read explanations for the spread of the current epidemic exactly along the lines you mention. The fact that these are all coastal countries makes a difference I’m guessing. All previous outbreaks occurred in very landlocked regions.
According to Reuters, the current outbreak mentioned by Dave in Congo has been confirmed Ebola, not ‘haemorrhagic gastritis’ as was claimed in the usual effort to stop ‘panic’. So add another likely hotspot with more than ~20 cases in another country.
There really is a large difference in the mortality & general behavior of the known strains, with the “Reston” strain apparently not lethal in humans. In one link I saw some retard claim that Ebola does not mutate, hahahhahahahaha, and yet discussed the various strains. What a maroon. Of course, it was immaculate conception.
Slow motion train wreck. I have a nice quote found when reading Albert Camus The Plague :
“A pestilence isn’t a thing made to man’s measure; therefore we tell ourselves that pestilence is a mere bogy of the mind, a bad dream that will pass away. But it doesn’t always pass away and, from one bad dream to another, it is men who pass away, and the humanists first of all, because they haven’t taken their precautions.”
Thanks for that info Bob, discouraging though it be. Obviously, we don’t need any more outbreaks right now.
Yes, no doubt the strains differ in virulence, Zaire and Sudan EBV being the highest and Reston the lowest.
Not only does EBV mutate, but since it’s a negative-strand RNA virus, it mutates fast because RNA-dependent RNA polymerases make many more mistakes than do DNA-dependent polymerases and there are no proofreading mechanisms as far as I know.
Pingback: Estimating the spread rate in the current ebola epidemic | Ecologically Orientated
One of the comment’s over on Zerohedge today (8-25-2014) made the observation that Rats are asymptomatic carriers of some strains of Ebola.
The quarantine of West Point in Monrovia is pointless if Rats eat the bodies of the Ebola killed and then act as a “co-living with humans” animal reserve of the disease.
Burning down West Point after the disease runs it course there would be even worse, as the Rats would flee into the rest of Monrovia.
The interaction of Ebola, Drug Addicts — who are by definition irrational when looking for their next drug fix — and Rats in densly populated areas in Western cities does not bear thinking…but we better hope somebody is screaming about that to WHO and the CDC.
I have not read anywhere that rats are known carriers. Fruit bats of several genera are the main reservoir, and other primates can get and transmit the disease. If you can provide a reference, that’s all I’m really interested in. I’ve got a couple and will try to check later.
We can imagine all sorts of disaster scenarios here but let’s please just stick to verifiable evidence as best we can determine it. People will say all kinds of things. I don’t want to fan any flames here, and certainly not start any new ones.
List of known carriers (which does include some rodents in a minor way) & other good source info on Ebola:
http://www.phac-aspc.gc.ca/lab-bio/res/psds-ftss/ebola-eng.php
This is the link from above that reports field rodent infection:
Morvan, J. M., Nakouné, E., Deubel, V., & Colyn, M. (2000). Ebola virus and forest ecosystem. [Écosystèmes forestiers et virus Ebola] Bulletin De La Societe De Pathologie Exotique, 93(3), 172-175.
Great, thanks Bob.
Another WordPress auto-approve failure btw, in case you were wondering.
ya, figured that and no problem re wordpress, and in any case, your blog, your rules ultimately.
Just by the by, we really have such little reliable data on Ebola and especially this outbreak that not much would surprise me coming out of this adaptive radiation….well, other than zombies & such trash. This is a whole new ballgame and certainly an immensely interesting textbook case for the now & future. I read and learn as I am able.
No matter what happens, it would appear that west Africa will now & always be another active locale for future outbreaks. How much further this territory extends may well be up to us since we are now the vector. Now most all of our species-community cloud has been newly exposed to this virus (dogs, rats. etc. noted w/ antibodies, etc) and who knows what will result. Sobering, isn’t it ?
Found another good discussion & source of links for Ebola technical & especially genetic history info:
http://www.flutrackers.com/forum/showthread.php?t=226864
eg. link to “EBOV is estimated to evolve at about 7×10-4 substitutions per site per year”
I appreciate your interest and the providing of the links Bob.
All the RNA viruses are fast mutaters as far as I know. Their polymerases make much higher copy errors.
The Congo outbreak is definitely another local outbreak from the known endemic local reservoir and has no likely link to the West Africa outbreak.